A. Limb salvage surgery
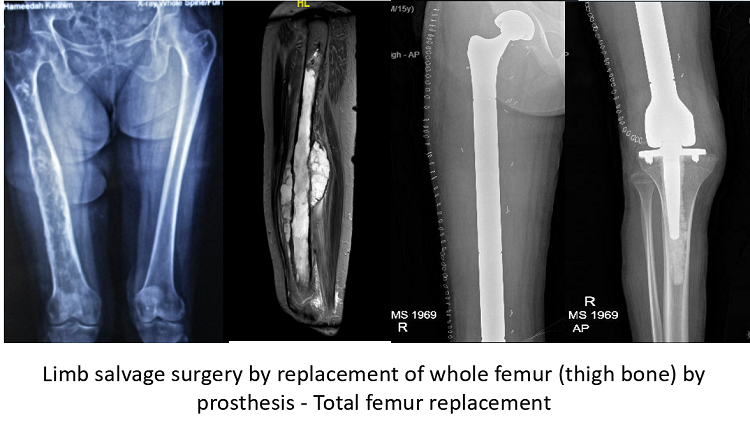
In the context of bone cancer, limb salvage surgery means preserving the limb, while completely removing the tumorous or cancerous portion of the bone. This is usually done with the intention of cure form cancer. More than 90 percent of patients with bone and muscle cancer undergo a limb saving surgery, and an amputation is very rarely required. There are three essential components of this surgery.
- Resection of tumor- This step involves complete removal the cancerous bone along with a cuff of normal tissue around the tumorå, making sure that enough muscles, nerves and vessels of the limb are saved so as to have a viable, functional limb. A careful pre operative assessment of the patient and the radiological investigations is crucial for successfully carrying out this step. Our attempt is be to save maximum soft tissue and bone, while ensuring complete cancer removal. If safely possible, the surgeon will try to save not just the limb, but also the joint and even the growth plate (in case of a growing child). We frequently rely on modern technologies like computer navigation and 3 D printed cutting jigs which bring the MRI and CT scan inputs directly on the surgeon’s cutting instruments. This ensures both complete disease removal and maximum function.
- Skeletal Reconstruction- After removing the tumor bearing bone, the surgeon will usually reconstruct the defect by one of the following means. A detailed discussion is needed to weigh the pros and cons of each method, before one of these is chosen.
A.) A metallic implant called a prosthesis. This is the most common means of reconstructing bone, quite often involving replacement of the joint also. There are many types of tumor prosthesis implants available, and the surgeon will discuss in detail about all options with the patient.
B). Sometimes, a bone graft is used to bridge the defect in the bone created by resection of the tumor. This graft may be taken form the patient’s own body or from a “bone bank”.
C). The bone which is cancerous may also be placed back from where it was removed, after killing all cancer in that bone by way of means like radiotherapy, cryosurgery etc.
- Soft tissue reconstruction- The muscles and skin are closed to adequately cover and give good functional support. Sometimes certain muscles flaps are also required.
• These are technically challenging surgeries done for rare indications and are best undertaken by surgeons experienced in performing these surgeries, mostly at centers with dedicated bone and soft tissue tumors departments.
• A detailed discussion with the surgeon is vital for successful outcome. The choice of surgery will depend, among a host of factors, on the patient’s age, location of tumor and the functional and occupational expectations. One should be aware of what lifestyle changes are recommended after limb salvage surgery with prosthesis.
• Postoperative physical therapy/ rehabilitation and compliance to the activity restrictions and instructions are extremely important for a successful outcome.
• The patient needs to be aware of any lifestyle modifications that are recommended after limb salvage surgery.
• Limb salvage surgery is a part of multidisciplinary management of bone cancers, and their outcome is interlinked with good pre and postoperative chemotherapy / radiation therapy, wherever indicated.
B. Extended Curettage
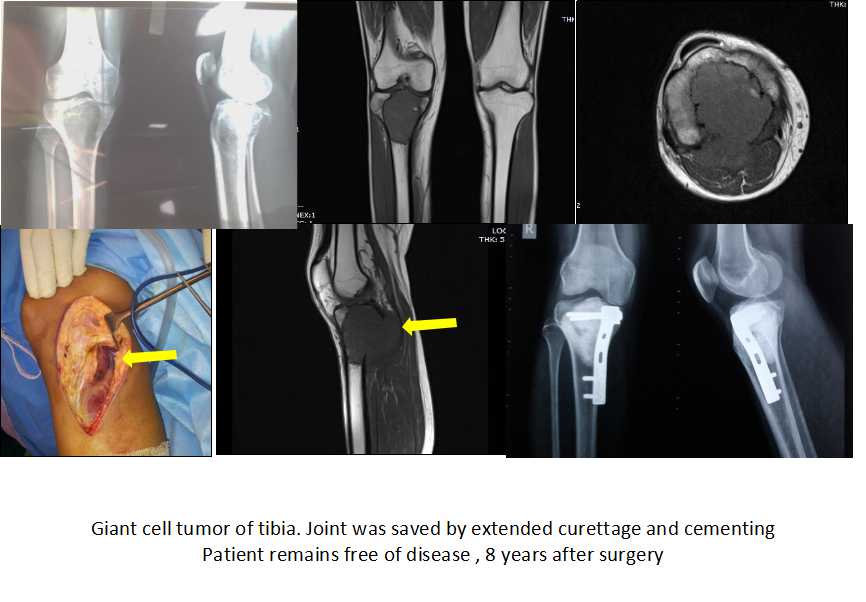
The most commonly recommended treatment of aggressive benign (non cancerous) bone tumors, of which giant cell tumor is the commonest, is curettage. Curettage is done after a careful preoperative evaluation which includes clinical examination, imaging in the form of x ray/ CT scan / MRI and biopsy. It involves thorough tumor removal while retaining the bony wall of the cavity which contained the tumor. The surgeon will then fill the cavity with bone cement/ bone graft/ bone graft substitute. This ensures long term control of disease in a vast majority of patients, while ensuring preservation of the patients’ own joint and bone and excellent limb function. There is no requirement of a prosthesis or a similar device. After surgery, clinicoradiological follow up is recommended.
• A good postoperative rehabilitation protocol is essential for a good outcome. Be sure of what exercises / precautions are to be followed.
• A good discussion with the surgeon is essential about the options of filling material, with their pros and cons.
• The advantages and disadvantages of resection as opposed to curettage is also part of preoperative counseling.
C. Amputation
A complete removal of the limb along with the whole of bone cancer, or amputation, is rarely needed nowadays. The surgeon will always carefully compare the pros and cons of limb salvage vs amputation, and discuss the same with the patient, before making a surgical plan.
D. Wide excision of soft tissue sarcoma
Like bone cancer, soft tissue sarcoma too has to be removed with a cuff of normal tissue. The vast majority of patients are offered limb saving surgeries. Here, too, the surgeon removes the complete tumor with a cuff of normal tissue. Quite often postoperative radiation therapy is required for soft tissue sarcoma. Where possible, a focused form of early postoperative radiotherapy called “Brachytherapy” is preferred. Sometimes plastic surgery is required for reconstruction of skin or muscle, and the musculoskeletal oncology team works closely with plastic and reconstructive surgery team to make a comprehensive plan of excisions and reconstruction. The plastic surgery team will often use local or regional flaps, or free flaps involving microvascular surgery by taking soft tissue from an area away from the site of tumor. The need and the options of plastic reconstructive surgery should be discussed in detail before the surgery.
• Any soft tissue swelling larger than 5 cm or located in deep tissues is to be investigated and considered a sarcoma unless proven otherwise.
• A timely intervention including early biopsy is vital to achieve optimal results.
• A multidisciplinary disease management group (DMG) consisting of orthopedic oncologist, musculoskeletal pathologist, musculoskeletal radiologist and medical and radiation and oncologists specializing in sarcoma management is essential for an optimal outcome of sarcoma management.

E. Biopsy
The diagnosis of all bone and soft tissue cancers and tumors are established by a procedure called biopsy. Here, a small piece if tissue is taken out of the tumor and sent for pathological examination. Any treatment will be started only after the final report of the biopsy is available. A properly performed biopsy is vital to a successful outcome and increases the chance of limb-salvage surgery. In fact, it is highly recommended that biopsies for bone and soft tissue tumors are done at centres where definitive limb salvage surgeries for bone and soft tissue sarcoma are routinely done. More than 90 % of biopsies are done as “Core needle biopsy”, which is a procedure done on and OPD basis, under local anaesthesia.
• A biopsy is an essential component of management of any bone cancer/ tumor. When properly performed at a specialized center, it does not harm the patient in any way.
• Biopsy for bone cancer should be done only at specialized centers where definitive management of these cancers, including limb salvages surgeries, are done
• The patient must consult the treating doctor as soon as the histopathology report is available, so that the correct treatment can be initiated.
• All guidelines recommend that bone and soft tissue tumors are managed at a center having a dedicated musculoskeletal (orthopedic) oncology disease management group (DMG). This group consists of an orthopedic oncologist, musculoskeletal pathologist, musculoskeletal radiologist and medical and radiation oncologists specializing in sarcoma management.